Written by:

SVP and Head of Research and Early Development, Respiratory and Immunology, AstraZeneca

Executive Director and Head of Bioscience Asthma and Skin Immunity, AstraZeneca
The interleukin 33 (IL-33) protein is a key regulator of immune response and tissue remodelling in chronic inflammatory diseases such as chronic obstructive pulmonary disease (COPD), asthma and diabetic kidney disease, as well as acute respiratory infections such as COVID-19. It has its effects through two distinct signalling mechanisms, one of which has only recently been discovered.
In order to protect us from illness, our immune system needs to detect and respond to a wide range of signals and triggers. Yet, while the acute responses of our immune system are vital for survival, extreme or persistent immune activation can become harmful and contributes to disease progression in various chronic illnesses including chronic obstructive pulmonary disease (COPD), asthma, atopic dermatitis and diabetic kidney disease. These illnesses affect over 600 million people1, with COPD being the third leading cause of death worldwide2. By understanding the science behind these diseases we’re exploring new ways to stop their progression, achieve remission and eventually cure them.
Also known as an alarmin, IL-33 is best known as a protein that acts as a cytokine to trigger a response from the immune system. It is found constitutively in the nucleus of numerous types of cell throughout the body including the lungs and skin. When these cells become damaged or die through necrosis, IL-33 is released and is able to interact with cells from the immune system. It acts on a range of cells including neutrophils, innate lymphoid cells, Th2 cells, eosinophils and mast cells via a receptor protein called ST2. IL-33 binding to ST2 triggers responses that lead to inflammation.
IL-33 in tissue remodelling
The form of IL-33 that exists inside cells and causes inflammation is known as reduced IL-33. Once released from cells, IL-33 is quickly converted into an oxidised form. Oxidised IL-33 doesn’t interact with ST2 and cannot cause inflammation, so the conversion of IL-33 limits the range of its effect.
Oxidised IL-33 has another role, however, which has recently been discovered. Oxidised IL-33 interacts with a different set of receptor proteins on the surface of epithelial cells3, the cells that form surfaces such as the linings of the airways in our lungs. In this role, IL-33 can trigger tissue remodelling changing how cells organise and specialise to perform different roles.
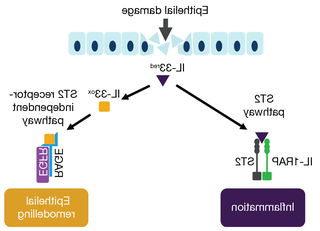
Oxidised IL-33 signals via RAGE/EGFR and ST2 pathways3,4
The role of IL-33 in chronic diseases
Our research has helped to show that IL-33 has a key role in several major illnesses and it is an attractive target for developing therapies.
Hallmarks of chronic lung diseases include changes to the cells that line the airways of the lungs, this includes an increase in cells mucus-producing goblet, which in turn leads to overproduction of mucus. Oxidised IL-33 may be a driver of the mucus overproduction that we see in COPD
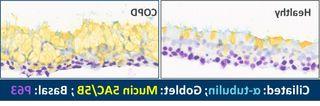
Oxidised IL-33 may be a driver of the mucus overproduction in COPD3
We are also working towards identification of patient subpopulations that may be particularly responsive to therapies that target IL-33, allowing for a precision medicine-led approach to treating these cases. Work is ongoing to uncover a suitable clinical test that can reliably identify these patients so that they can be matched to precision medicines which they are most likely to benefit from
The challenge of complex diseases
Chronic diseases are difficult to treat and manage because they are highly heterogeneous, varying between patients as well as over time and in response to a wide range of external factors. There is still a huge amount we do not understand about these illnesses but, by following the science, we are learning more about the pathogenesis and uncovering new targets to help manage and ultimately cure these diseases.

